Prevention
Modern medicine is increasingly transitioning towards preventive care. This shift towards prevention has also been observed in breast cancer care in recent years, particularly with the discovery of the BRCA gene. Subsequently, multiple genes and risk factors have been identified. Depending on these factors, a personalized screening strategy can be chosen. Therefore, it is crucial to understand these genetic and risk factors.
Diagnosis
I was diagnosed with cancer ... This website serves as a portal designed to assist you and your loved ones in accessing personal information and finding solutions to your concerns.
The primary goal of this website is to offer guidance and support to patients as they navigate their journey toward recovery and improved quality of life. The "Diagnosis" section of our website is divided into two main categories. Firstly, under "Anatomy and Physiology," we provide fundamental knowledge about the breast. Secondly, in the "Tumors and Disorders" section, we delve deeper into various breast-related conditions.
Moreover, we aim to provide information to women who may be concerned about potential breast issues but are hesitant to seek immediate medical advice. Knowledge and information can often offer immediate reassurance if a woman is able to identify the issue herself and determine that no specific treatment is necessary. Conversely, we also strive to educate women who have received a diagnosis of a serious breast condition, such as breast cancer, and wish to approach their doctor well-informed and prepared.
Treatment
The treatment for breast cancer should immediately include a discussion about reconstruction. Our foundation has no greater goal than to raise awareness of this among patients and oncological surgeons. By making an informed decision beforehand, we avoid closing off options for later reconstruction while still considering the oncological aspect. Of course, survival is paramount, and the decision of the oncologic surgeon will always take precedence.
The "Reconstruction or not?" page contains all the information you can expect during an initial consultation before undergoing tumor removal. This page is comprehensive, and your plastic surgeon will only provide information relevant to your situation.
"Removing the tumor" details the surgical procedure itself. This is the most crucial operation because effective tumor removal remains paramount. We guide you through the various methods of removal, a decision often made by a multidisciplinary team comprising oncologists, radiologists, pathologists, radiotherapists, breast nurses, gynecologists, oncological surgeons, and plastic surgeons.
The "Breast Reconstruction" section includes information and illustrations of the different reconstruction options along with corresponding steps.
Revalidation
Those treated for cancer often need a long period to recover.
Cancer is a radical illness with a heavy treatment. Often, people have to deal with psychosocial and/or physical problems afterwards, such as stress, anxiety, extreme fatigue, painful joints, reduced fitness, lymphedema... This can have a major impact on general well-being.
There are rehabilitation programmes offered by most hospitals. We cover some of the major topics here.
Quality of life
Quality of life is a key factor in coping with breast cancer. Therefore, it is important to find coping mechanisms that work, which will be different from patient to patient. For some, it may be finding enjoyment in activities they engaged in prior to diagnosis, taking time for appreciating life and expressing gratitude, volunteering, physical exercise... Of prime importance, studies have shown that accepting the disease as a part of one’s life is a key to effective coping, as well as focusing on mental strength to allow the patient to move on with life. In this section we are addressing some topics that patients experience during and after treatment and we are providing information to address them.
Surgical and anatomical details of the breast
The 3-step principle
The 3-step principle of breast analysis was developed to help describe and deal with complex deformities of the female breast. It divides the breast into 3 simple anatomical features; the footprint, the conus and the skin envelope.
Applying the 3-step principle greatly simplifies surgical planning and management.
1. The footprint
The footprint is the outline of the breast base on the chest wall and is the interface of the posterior surface of the breast with the thoracic cavity. The footprint forms the foundation of the overlying three-dimensional structure of the breast (fig. 1).
The footprint can easily be seen at the end of a mastectomy, if the overlying skin is retracted, exposing the serratus anterior and pectoral muscles.
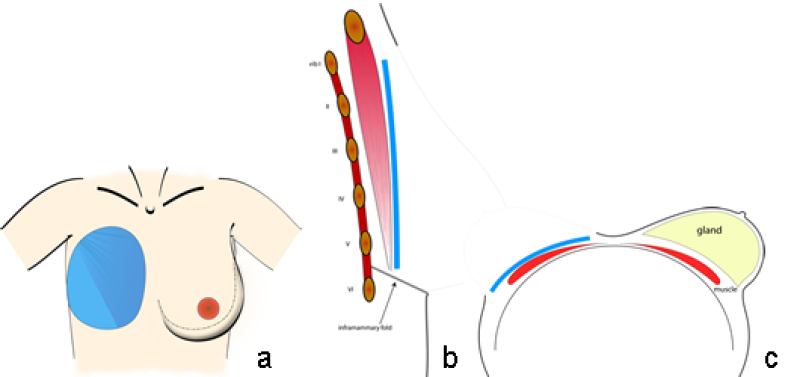
Fig. 1: Typical size and position of the breast footprint on the chest wall on a frontal (a) sagittal standing (b) and an axial supine view (c).
2. The conus
The conus refers to the three dimensional shape, projection and volume of the breast. It is normally formed by the mammary gland and sits anterior to the footprint of the breast (fig. 2). Each conus has a specific volume and yet its composition is different in every individual woman. The base of the conus corresponds to, or is slightly smaller than, the breast footprint. In a standing position, there is a gradual transition of the chest wall into the upper and medial aspects of the female breast. The infraclavicular area is typically flat or even slightly concave. This transition at the lateral and inferior part of a normal breast is sharper and may even reach 180° at the lower border of hypertrophic or severely ptotic breasts. The conus typically has lower lateral fullness, a maximum projection at the level of the nipple-areolar complex just lateral to the mid-clavicular line and a varying degree of ptosis.
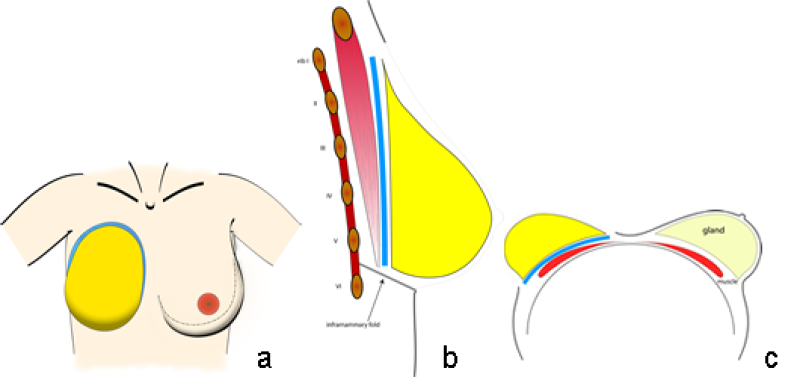
Fig. 2: Typical size and position of the footprint (blue) and the conus (yellow) of the breast on the chest wall in a frontal (a) sagittal standing (b) and an axial supine view (c).
3. The skin envelope
The skin envelope is the overlying skin and subcutaneous fat of the breast (fig. 3). Normally the skin envelope functions like a well-fitting brassiere, holding the conus in position and aiding projection.
The interface between the skin envelope and the conus can play an important role in breast shape. Scarring, due to surgery or radiotherapy, can tighten the envelope, while stretching of Cooper’s ligament or the superficial layer of the superficial fascia can loosen this envelope.
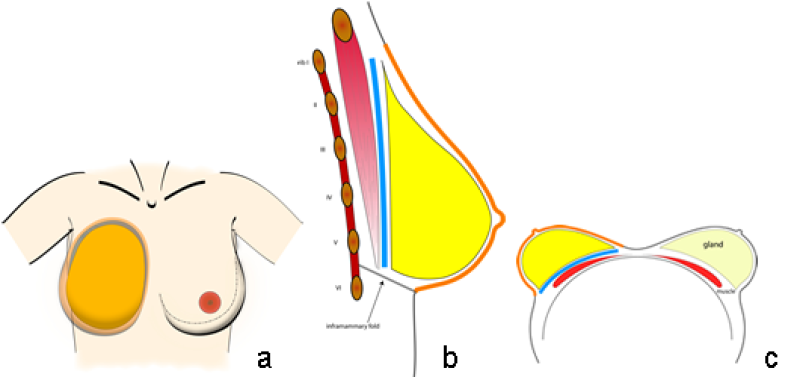
Fig. 3: Typical size and position of the footprint (blue), the conus (yellow) and the skin envelope (orange) of the breast on the chest wall in a frontal (a) sagittal standing (b) and an axial supine view (c).
The nipple-areolar complex (NAC) is also a component of the skin envelope. It contributes to the overall aesthetic appearance of the breast, by highlighting the point of maximal anterior-posterior projection, along either the vertical meridian line or slightly lateral to it (fig. 4). An attractive areola is pigmented, has a conical shape and is a smooth continuation of the natural contour of the skin envelope of the breast. The nipple protrudes above the areola. Nipple-areolar complex color and nipple dimensions are subject to wide variation and individual preference.
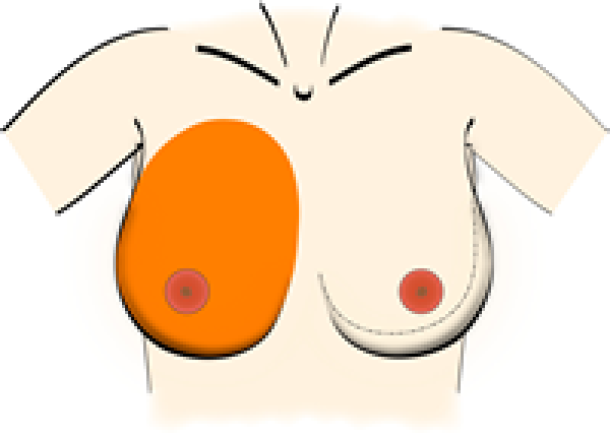
Fig. 4: The nipple-areolar complex (NAC) sits at the point of maximal anterior-posterior projection of the breast, either along the vertical meridian line or just slightly lateral to it.
The final breast shape is not determined independently by the footprint, the conus or the skin envelope. It is the interaction of these 3 elements that contributes to the maintenance of a pleasing, natural-looking breast over time.
References
Shaping the breast in aesthetic and reconstructive breast surgery: an easy three-step principle.
Blondeel PN, Hijjawi J, Depypere H, Roche N, Van Landuyt K. Plast Reconstr Surg. 2009 Feb;123(2):455-62.
Shaping the breast in aesthetic and reconstructive breast surgery: an easy three-step principle. Part II–Breast reconstruction after total mastectomy.
Blondeel PN, Hijjawi J, Depypere H, Roche N, Van Landuyt K. Plast Reconstr Surg. 2009 Mar;123(3):794-805.
Shaping the breast in aesthetic and reconstructive breast surgery: an easy three-step principle. Part III–reconstruction following breast conservative treatment.
Blondeel PN, Hijjawi J, Depypere H, Roche N, Van Landuyt K. Plast Reconstr Surg. 2009 Jul;124(1):28-38.
Discussion. Shaping the breast in aesthetic and reconstructive breast surgery: an easy three-step principle. Part III–reconstruction following breast conservative treatment.
Nahabedian MY. Plast Reconstr Surg. 2009 Jul;124(1):39-40.
Discussion. Shaping the breast in aesthetic and reconstructive breast surgery: an easy three-step principle. Part III–reconstruction following breast conservative treatment.
Hammond DC. Plast Reconstr Surg. 2009 Jul;124(1):41-2.
Discussion. Shaping the breast in aesthetic and reconstructive breast surgery: an easy three-step principle. Part IV–aesthetic breast surgery.
Hammond DC. Plast Reconstr Surg. 2009 Aug;124(2):385-6.
Shaping the breast in aesthetic and reconstructive breast surgery: an easy three-step principle. Part IV–aesthetic breast surgery.
Blondeel PN, Hijjawi J, Depypere H, Roche N, Van Landuyt K. Plast Reconstr Surg. 2009 Aug;124(2):372-82.
Discussion. Shaping the breast in aesthetic and reconstructive breast surgery: an easy three-step principle. Part IV–aesthetic breast surgery.
Nahabedian MY. Plast Reconstr Surg. 2009 Aug;124(2):383-4.