Prevention
Modern medicine is increasingly transitioning towards preventive care. This shift towards prevention has also been observed in breast cancer care in recent years, particularly with the discovery of the BRCA gene. Subsequently, multiple genes and risk factors have been identified. Depending on these factors, a personalized screening strategy can be chosen. Therefore, it is crucial to understand these genetic and risk factors.
Diagnosis
I was diagnosed with cancer ... This website serves as a portal designed to assist you and your loved ones in accessing personal information and finding solutions to your concerns.
The primary goal of this website is to offer guidance and support to patients as they navigate their journey toward recovery and improved quality of life. The "Diagnosis" section of our website is divided into two main categories. Firstly, under "Anatomy and Physiology," we provide fundamental knowledge about the breast. Secondly, in the "Tumors and Disorders" section, we delve deeper into various breast-related conditions.
Moreover, we aim to provide information to women who may be concerned about potential breast issues but are hesitant to seek immediate medical advice. Knowledge and information can often offer immediate reassurance if a woman is able to identify the issue herself and determine that no specific treatment is necessary. Conversely, we also strive to educate women who have received a diagnosis of a serious breast condition, such as breast cancer, and wish to approach their doctor well-informed and prepared.
Treatment
The treatment for breast cancer should immediately include a discussion about reconstruction. Our foundation has no greater goal than to raise awareness of this among patients and oncological surgeons. By making an informed decision beforehand, we avoid closing off options for later reconstruction while still considering the oncological aspect. Of course, survival is paramount, and the decision of the oncologic surgeon will always take precedence.
The "Reconstruction or not?" page contains all the information you can expect during an initial consultation before undergoing tumor removal. This page is comprehensive, and your plastic surgeon will only provide information relevant to your situation.
"Removing the tumor" details the surgical procedure itself. This is the most crucial operation because effective tumor removal remains paramount. We guide you through the various methods of removal, a decision often made by a multidisciplinary team comprising oncologists, radiologists, pathologists, radiotherapists, breast nurses, gynecologists, oncological surgeons, and plastic surgeons.
The "Breast Reconstruction" section includes information and illustrations of the different reconstruction options along with corresponding steps.
Revalidation
Those treated for cancer often need a long period to recover.
Cancer is a radical illness with a heavy treatment. Often, people have to deal with psychosocial and/or physical problems afterwards, such as stress, anxiety, extreme fatigue, painful joints, reduced fitness, lymphedema... This can have a major impact on general well-being.
There are rehabilitation programmes offered by most hospitals. We cover some of the major topics here.
Quality of life
Quality of life is a key factor in coping with breast cancer. Therefore, it is important to find coping mechanisms that work, which will be different from patient to patient. For some, it may be finding enjoyment in activities they engaged in prior to diagnosis, taking time for appreciating life and expressing gratitude, volunteering, physical exercise... Of prime importance, studies have shown that accepting the disease as a part of one’s life is a key to effective coping, as well as focusing on mental strength to allow the patient to move on with life. In this section we are addressing some topics that patients experience during and after treatment and we are providing information to address them.
Tumorectomy
A benign tumor does not have the ability to spread to distant organs and therefore can be completely excised. As it grows, it pushes away breast tissue and usually has a clear boundary around it. The goal of surgery is to remove the tumour but none of the surrounding normal breast tissue.
Removing a malignant tumor is different. A malignant tumor has fine offshoots that grow in all directions. These resemble the tentacles of an octopus. This boundary is often difficult to determine but it is essential to completely remove a malignant tumor. To ensure that the tumor and all its possible extensions are excised, a wide margin of surrounding normal tissue has to be removed.
The excised tissue is then examined under a microscope to check that all the offshoots have been removed. The edge of the removed breast tissue specimen is called the ‘tumor free resection zone’ or ‘tumor-free margin’.
Before undertaking a surgical procedure to remove the tumor, the exact nature and extent of the tumor should be determined to help plan surgery and fully inform the patient. All the possible alternatives to treat the tumor should be explained.
The removal of a breast tumor depends on its nature . The difference between a benign lesion and a breast cancer can be determined by physical examination and imaging of the tumor by mammography and ultrasound.
Ultimately, in all patients, confirmation of the diagnosis should be obtained before surgery by removing a small portion of the tumor and sending it for microscopic examination.
This is mostly done by needle biopsy:
With fine needle aspiration, cells that are aspirated can be examined under the microscope.
The most accurate method of histological diagnosis is a cylindrical biopsy. This is harvested using a slightly larger needle. This enables a more detailed microscopic examination and therefore accurate diagnosis.
A mammotome is a vacuum assisted breast biopsy device that uses X-ray, ultrasound or MRI to perform a small breast biopsy. A mammotome biopsy can be done under local anesthesia and removes only a small amount of healthy tissue.
If the tumor is detected early and is small, only the tumor itself and a limited rim of healthy tissue of the breast may need to be removed. This surgical procedure is called a tumorectomy (fig. 1).

figure 1a: status after biopsy (fresh scar around the areola) of a tumor recurrence after a wide tumorectomy in the lower-inner quadrant of the right breast. Shape and volume asymmetry are visible but not grossly disturbing.

figure 1b: status after tumorectomy in the upper-inner quadrant of the right breast. Shape and volume asymmetry are visible but not grossly disturbing.
Incisions can be made over the tumor or at more concealed locations like the edge of the areola or within the crease below the breast (figure 2). After removal of the tumor, it will be examined histologically.
Fig. 2: possible incisions in the breast depending on size and location of the tumor. It is very important to position the incisions within the limits of the bra-line (first drawing).
Using mammographic screening, which is supported by most European Countries, small tumors that cannot be felt from outside can be detected. These tumors are often not palpable and so their removal is performed by needle localisation. Pre-operatively, a wire is placed by a radiologist to identify the site of the tumor (fig. 3a). At surgery, the wire is traced and the tissue at the tip of the wire is excised. The tissue with wire in situ are then sent back to the radiologist, while the patient is kept under anesthesia. The radiologist takes an X-ray to confirm that the correct area has been removed (fig. 3b).
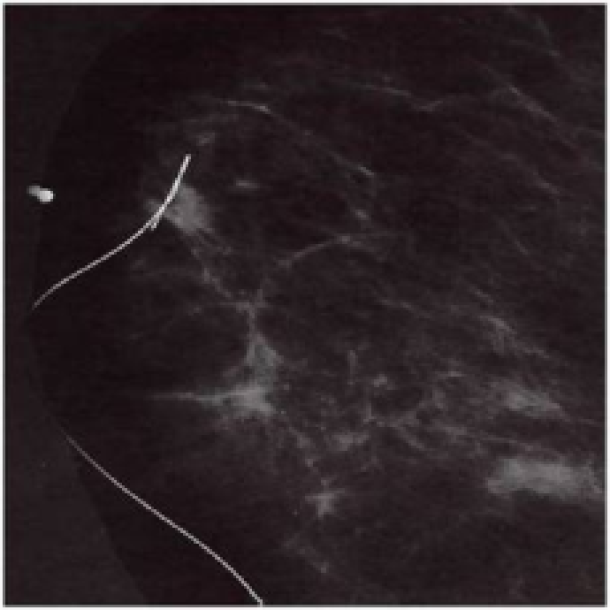
Figure 3a: mammogram with needle localization of a non palpable tumor.
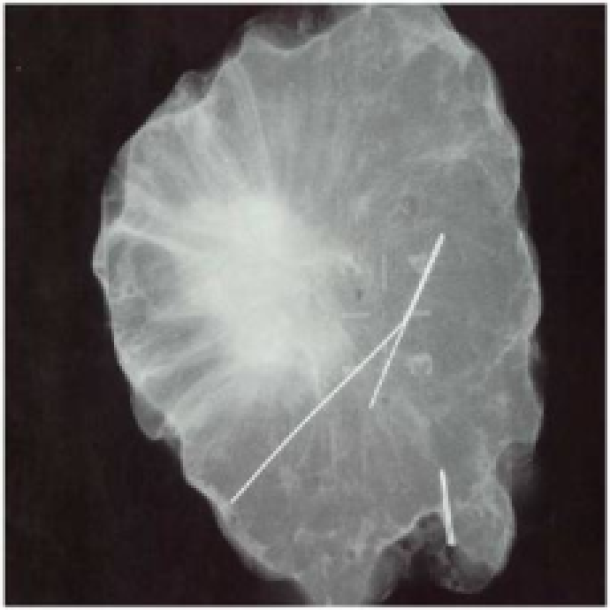
Figure 3b: X-ray of the same tumor after resection of both the tumor and wire.
If the wire indicates that the tumor is in the center specimen, one can be certain that it has been removed with a sufficient tumor-free margin. If the tumor is however close to one edge of the specimen, some additional breast tissue can be removed (wider excision) while the patient remains asleep.
If, after tumorectomy, the aesthetic appearance of the breast is affected, breast reconstruction may be indicated. Today small defects can easily be corrected by simple lipofilling. The different methods of breast reconstruction are discussed in other areas of this website.
References
Consensus conference on breast conservation.
Schwartz GF, Veronesi U, Clough KB, Dixon JM, Fentiman IS, Heywang-Köbrunner SH, Holland R, Hughes KS, Mansel RE, Margolese R, Mendelson EB, Olivotto IA, Palazzo JP, Solin LJ; Consensus Conference Committee. J Am Coll Surg. 2006 Aug;203(2):198-207.
Outcome of breast-conserving therapy in the Tokyo Women’s Medical University Breast Cancer Society experience.
Karasawa K, Obara T, Shimizu T, Haga S, Okamoto T, Ito Y, Kamio T, Kimura T, Kameoka S, Mitsuhashi N, Nishikawa T, Aiba M, Izuo M. Breast Cancer. 2003;10(4):341-8.
Integration of plastic surgery in the course of breast-conserving surgery for cancer to improve cosmetic results and radicality of tumor excision.
Petit JY, Rietjens M, Garusi C, Greuze M, Perry C. Recent Results Cancer Res. 1998;152:202-11.
Ten year results of a randomised trial comparing two conservative treatment strategies for small size breast cancer.
Mariani L, Salvadori B, Marubini E, Conti AR, Rovini D, Cusumano F, Rosolin T, Andreola S, Zucali R, Rilke F, Veronesi U. Eur J Cancer. 1998 Jul;34(8):1156-62.
Breast-conserving treatment: controversies and consensus.
Noguchi M, Kinne DW, Miyazaki I. J Surg Oncol. 1996 Jul;62(3):228-34.
Controversies in the local management of invasive and non-invasive breast cancer.
Page DL, Johnson JE. Cancer Lett. 1995 Mar 23;90(1):91-6.