Prevention
Modern medicine is increasingly transitioning towards preventive care. This shift towards prevention has also been observed in breast cancer care in recent years, particularly with the discovery of the BRCA gene. Subsequently, multiple genes and risk factors have been identified. Depending on these factors, a personalized screening strategy can be chosen. Therefore, it is crucial to understand these genetic and risk factors.
Diagnosis
I was diagnosed with cancer ... This website serves as a portal designed to assist you and your loved ones in accessing personal information and finding solutions to your concerns.
The primary goal of this website is to offer guidance and support to patients as they navigate their journey toward recovery and improved quality of life. The "Diagnosis" section of our website is divided into two main categories. Firstly, under "Anatomy and Physiology," we provide fundamental knowledge about the breast. Secondly, in the "Tumors and Disorders" section, we delve deeper into various breast-related conditions.
Moreover, we aim to provide information to women who may be concerned about potential breast issues but are hesitant to seek immediate medical advice. Knowledge and information can often offer immediate reassurance if a woman is able to identify the issue herself and determine that no specific treatment is necessary. Conversely, we also strive to educate women who have received a diagnosis of a serious breast condition, such as breast cancer, and wish to approach their doctor well-informed and prepared.
Treatment
The treatment for breast cancer should immediately include a discussion about reconstruction. Our foundation has no greater goal than to raise awareness of this among patients and oncological surgeons. By making an informed decision beforehand, we avoid closing off options for later reconstruction while still considering the oncological aspect. Of course, survival is paramount, and the decision of the oncologic surgeon will always take precedence.
The "Reconstruction or not?" page contains all the information you can expect during an initial consultation before undergoing tumor removal. This page is comprehensive, and your plastic surgeon will only provide information relevant to your situation.
"Removing the tumor" details the surgical procedure itself. This is the most crucial operation because effective tumor removal remains paramount. We guide you through the various methods of removal, a decision often made by a multidisciplinary team comprising oncologists, radiologists, pathologists, radiotherapists, breast nurses, gynecologists, oncological surgeons, and plastic surgeons.
The "Breast Reconstruction" section includes information and illustrations of the different reconstruction options along with corresponding steps.
Revalidation
Those treated for cancer often need a long period to recover.
Cancer is a radical illness with a heavy treatment. Often, people have to deal with psychosocial and/or physical problems afterwards, such as stress, anxiety, extreme fatigue, painful joints, reduced fitness, lymphedema... This can have a major impact on general well-being.
There are rehabilitation programmes offered by most hospitals. We cover some of the major topics here.
Quality of life
Quality of life is a key factor in coping with breast cancer. Therefore, it is important to find coping mechanisms that work, which will be different from patient to patient. For some, it may be finding enjoyment in activities they engaged in prior to diagnosis, taking time for appreciating life and expressing gratitude, volunteering, physical exercise... Of prime importance, studies have shown that accepting the disease as a part of one’s life is a key to effective coping, as well as focusing on mental strength to allow the patient to move on with life. In this section we are addressing some topics that patients experience during and after treatment and we are providing information to address them.
Anatomy
The normal appearance of a breast
What does a normal breast look like? Watch the following video by Laura Dodsworth:
Development of the breast
During fetal development, the breast first arises as a pigmented nipple elevation of the chest skin, on each side of the sternum. The breast ducts are formed by an invagination of these nipples. The milk duct structure and the nipple of the breast are present at the time of birth. The breast glands develop during puberty under the influence of hormones. During this period, they are also surrounded by more fat which contributes to the final adult volume and shape. During pregnancy, the glands are temporary activated to produce milk by hormone stimulation. During menopause the breasts atrophy and decrease in volume.
Structure of the breast
In the anatomical position, the female breast lies at the level of the second to the sixth rib. The breast covers a large part of the pectoralis major muscle. The breast can be considered in terms of its volume and its skin envelope. The skin envelope is partly responsible for the shape of the breast.
The nipple and areola are important features at the ‘top’ of the breast. Both contain pigments. The areola is usually round. The nipple is located centrally in the areola. Randomly distributed around it, small pale coloured bumps can be found called Montgomery glands. They produce sebum. In some circumstances, they may lead to a cyst.
The female breast is composed of approximately 15 to 20 lobes. Each lobe is made up of many smaller lobules where under certain hormonal conditions milk can be produced. The milk duct collects the milk from the lobules and carries it to the nipple. The lobes are embedded in adipose tissue and are separated by fibrous membranes which are attached to the underlying muscle, holding the entire structure together. These fibrous membranes are the ligaments of Astley Cooper. Together the skin, the adipose tissue around the glands and the glands themselves, determine the overall shape of the breast.
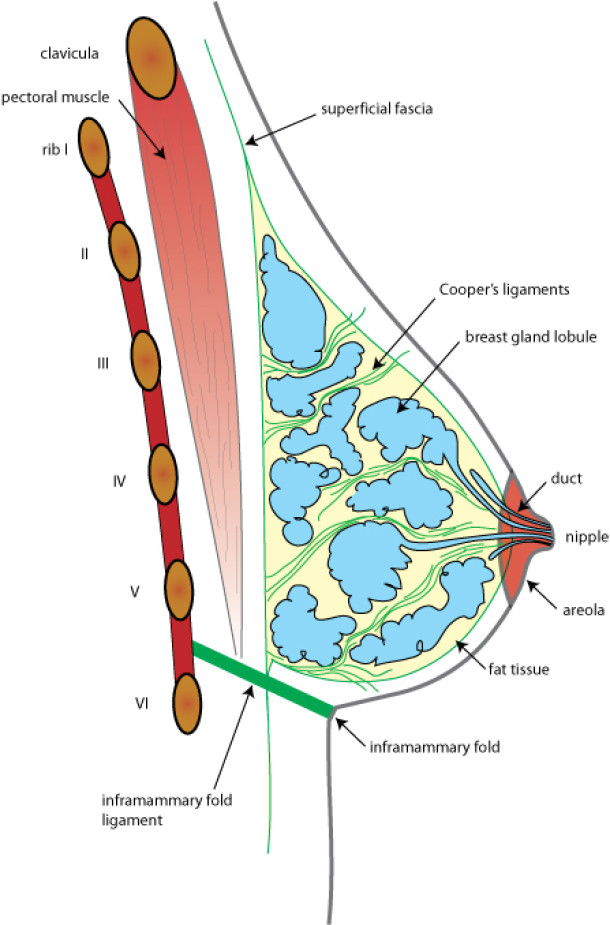
Fig. 1. Composition of the breast: glandular tissue (blue), fat (yellow) and connective tissue strands (green) are contained between two sheets of the superficial fascia, a tough connective tissue layer that surrounds the entire body. A strong ligament determines the position and shape of the inframammary fold. The chest is separated from the underlying pectoralis major by a network of loose connective tissue.
Blood supply of the breast
The breast has a rich blood supply from a number of different sources. The main supply is from an artery that originates in the armpit. There is an additional supply from both the internal throracic arteries (originating near the sternum) and from the arteries of the ribs.
Drainage is through a network of veins which follow a similar pattern to the arteries and, additionally, through a complex framework of superficial veins just under the skin. Many of these veins are visible to the naked eye.
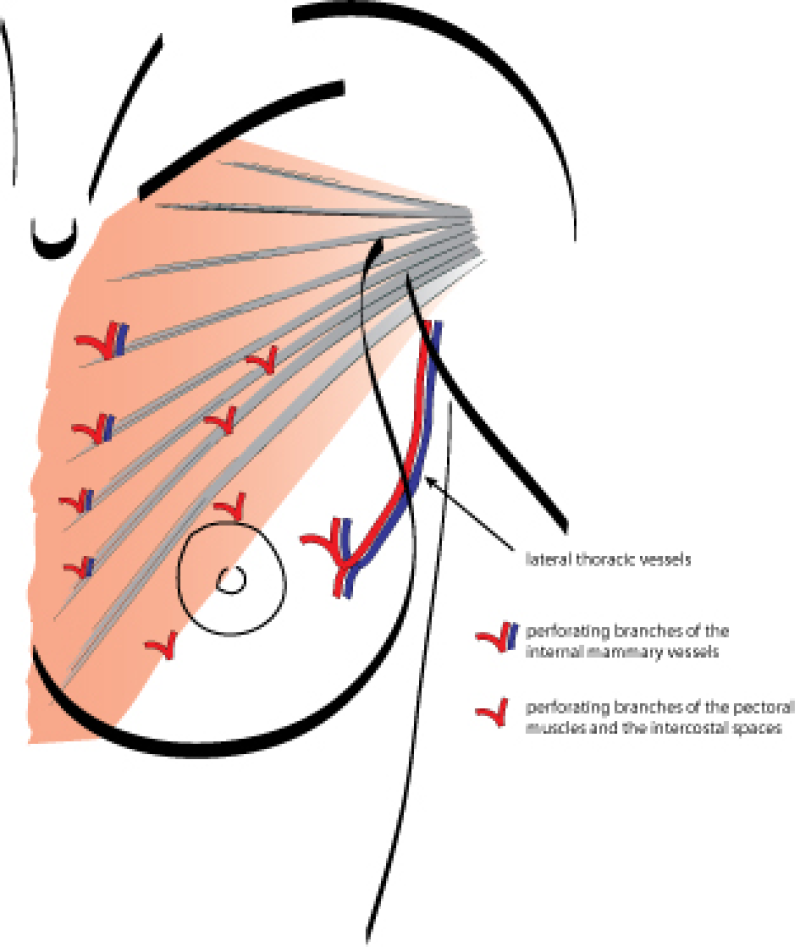

Left: The breast arteries (red) and veins (blue) provide an extensive network of blood vessels.
Right: Superficial veins are typically visible in the normal breast.
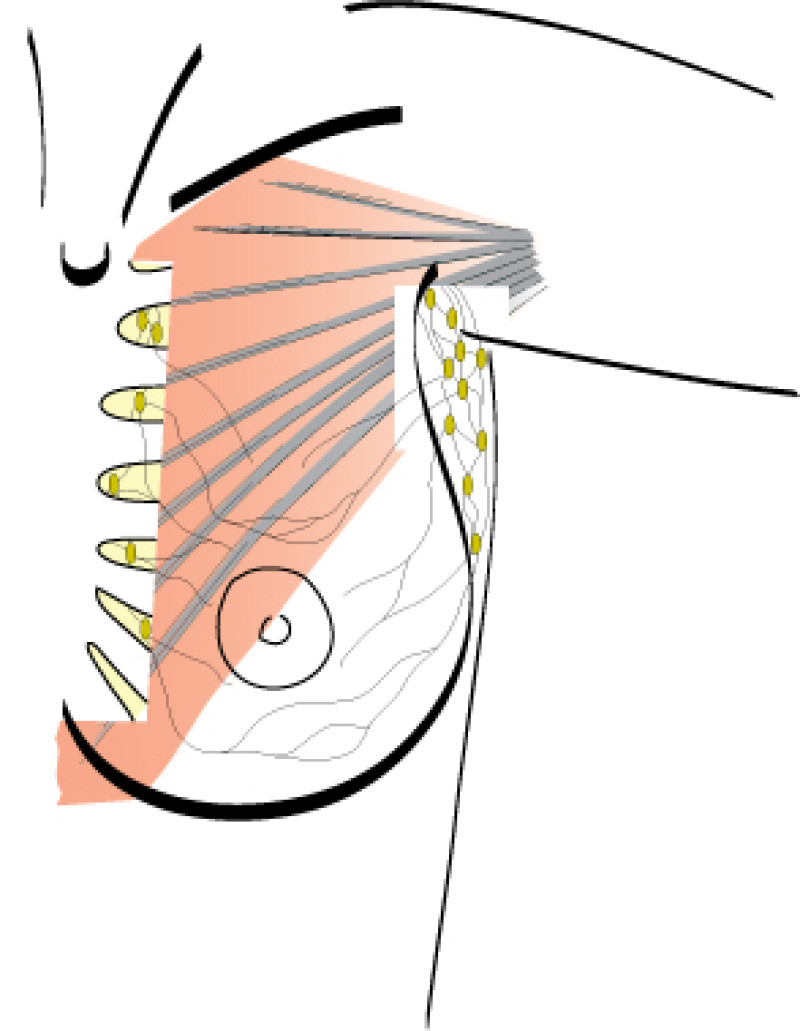
Lymphatic drainage
The lymphatic drainage of the breast is an equally large network and plays an important role in breast cancer. Much of the lymph is drained from the outer chest wall to the lymph nodes within the armpit (approximately 20 to 30 ‘axillary’ lymph nodes). The remaining lymph is drained towards the midline, to the lymph nodes in the region of the sternum (parasternal nodes). The two axillary lymph node regions are connected with each other via a lymphatic network across the chest. The lymph then flows from here to beneath the collarbone and the base of the neck. There is a direct connection to the large veins that run back to the heart. In some rare cases there is also direct drainage to the mediastinum, liver, parasternal and axillary lymph nodes from the other side and along the ribs.
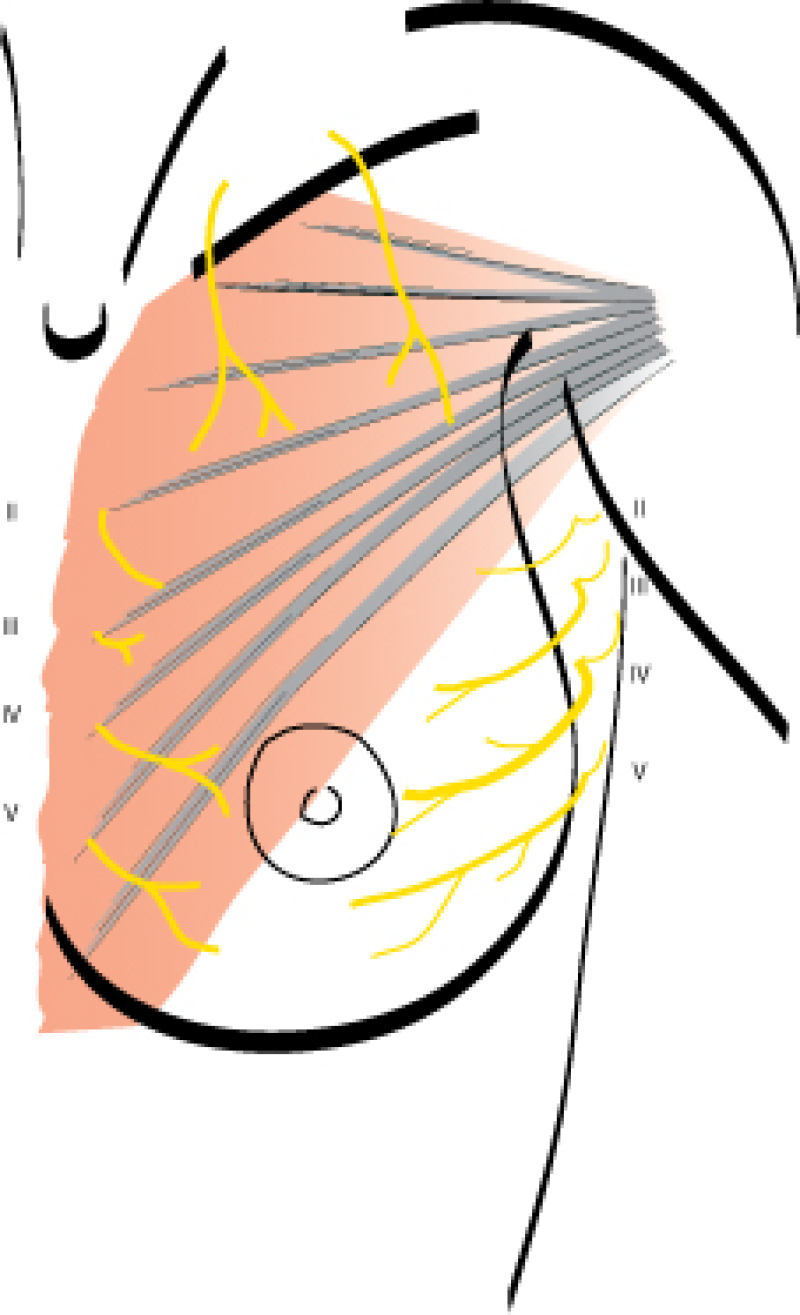
Innervation
Sensation to the breast skin is supplied by nerves that run horizontally from the sides towards the center of the chest between the 2nd to the 6th ribs. The nerve at the level between the 4th and 5th rib is especially important as it provides sensation to the nipple and areola. The upper areas of the breast are innervated by superficial nerves coming down from the base of the neck.